VSD
Definition
A defect in the ventricular septum allowing communication between the RV and LV. It is the most common congenital heart defect (excluding bicuspid aortic valve).
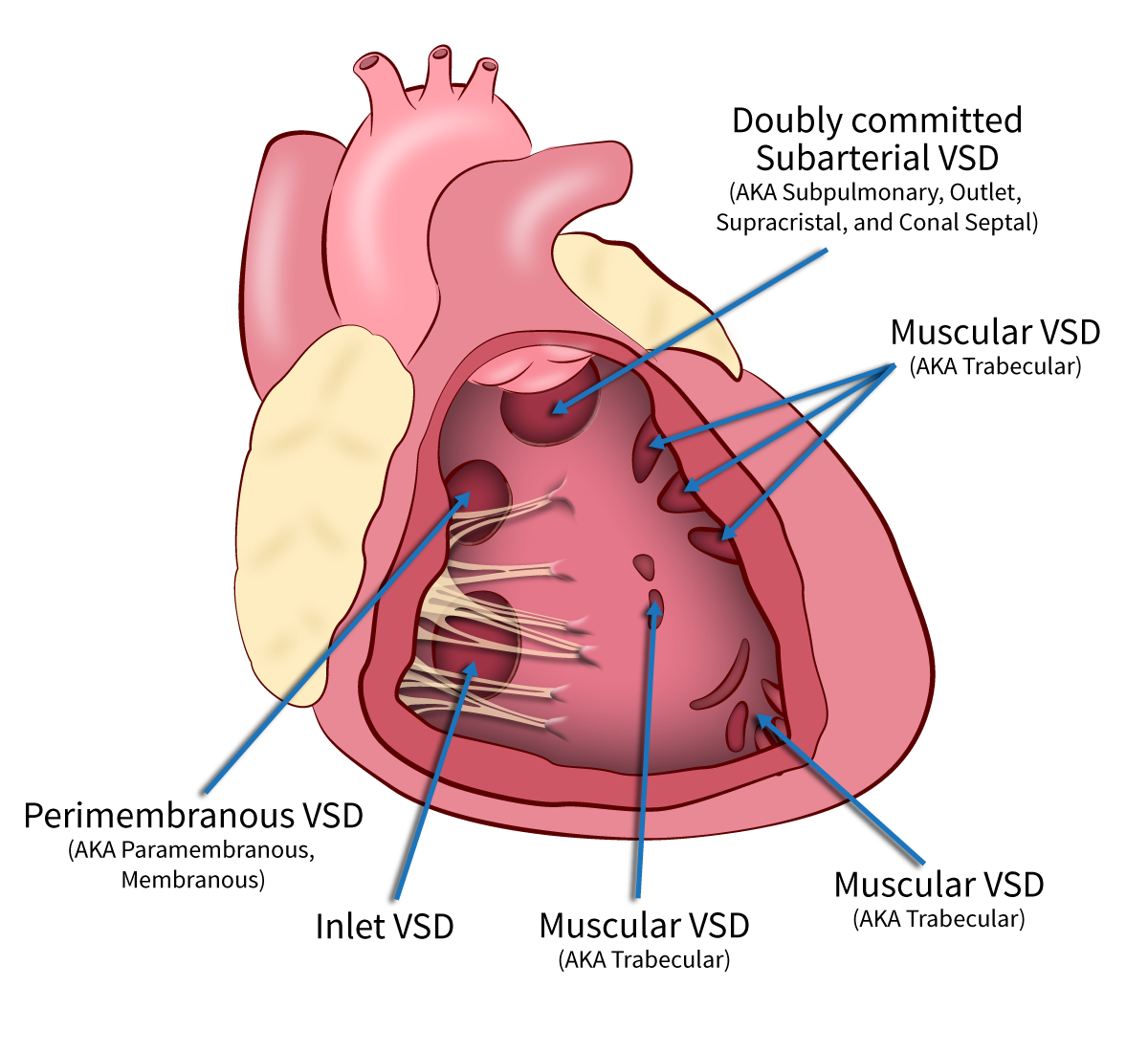
1. Classification
- Membranous (70%): In the upper septum, near the aortic valve.
- Muscular (20%): In the trabecular septum ("Swiss cheese" appearance if multiple).
- Inlet (Posterior): Near the tricuspid valve (common in Down Syndrome/AVSD).
- Outlet (Supracristal/Subarterial): Beneath pulmonary valve (associated with Aortic Regurgitation).
2. Hemodynamics
- Left-to-Right Shunt: Blood flows from high-pressure LV to low-pressure RV.
- Volume Overload: Increased flow to Pulmonary Artery
Lungs LA LV.
Key Concept
VSD causes volume overload of the Left Atrium and Left Ventricle (and RV pumping against pressure, not volume, unless huge).
3. Clinical Features
| Size Category | Absolute Diameter | Relative to Aortic Root / Annulus | Hemodynamic Status | Shunt Magnitude (Qp:Qs) |
|---|---|---|---|---|
| Very Small / Small | < 5 mm | VSD to Aorta ratio < 0.5 | Pressure restrictive | < 1.5:1 |
| Moderate (Medium) | 5 – 10 mm | VSD to Aorta ratio ≈ 1 | Moderately restrictive | 1.5:1 – 2:1 |
| Large | > 10 mm | > 50% of Aortic diameter, or ≥ Aortic annulus | Non-restrictive | > 2:1 |
- Symptoms: Tachypnea, diaphoresis during feeds, failure to thrive, recurrent chest infections.
4. Physical Examination
- Palpation: Hyperdynamic precordium, Systolic Thrill at LLSB.
- Auscultation:
- Murmur: Harsh, Pansystolic Murmur best heard at Left Lower Sternal Border (LLSB).
- Pearl: Intensity is inversely proportional to size (Small VSD = Loud Murmur).
- P2: Loud (if Pulmonary Hypertension develops).
- Mid-diastolic rumble: At apex (due to increased flow across Mitral valve in large VSDs).
5. Investigations
- CXR: Cardiomegaly (LV type), Pulmonary Plethora (increased vascular markings).
- ECG:
- QRS Small to Normal.
- Large: Left Atrial Enlargement (LAE) and Biventricular Hypertrophy (BVH).
- Classic Sign: Katz-Wachtel Phenomenon (Large equiphasic QRS complexes in V2-V5).
- Echo: Diagnostic (location, size, gradient).
6. Management
A. Medical
- Treat Congestive Heart Failure: Diuretics (Furosemide), ACE Inhibitors (Enalapril).
- Nutritional support (high-calorie feeds).
- Treat infections.
B. Surgical/Interventional
- Indications for Closure:
- Uncontrolled CHF / Failure to thrive.
- Qp:Qs > 2:1.
- Development of Pulmonary Hypertension (pre-Eisenmenger).
- Supracristal VSD with Aortic Regurgitation (prolapse of right coronary cusp).
- Methods:
- Surgical Patch Closure: (Dacron/Gore-tex) - Gold standard.
- Transcatheter Device Closure: For suitable Muscular VSDs.
C. Natural History
- 30-50% of small membranous/muscular VSDs close spontaneously in the first 2 years.